Key Takeaways: HIPAA-compliant file sharing requires end-to-end encryption, access controls, audit trails, and signed Business Associate Agreements. This article is for healthcare providers, practice administrators, compliance officers, and anyone handling protected health information who needs to understand secure sharing requirements.
Why Healthcare File Sharing Demands Special Attention
Healthcare organizations share more digital files today than ever before. Imaging studies travel from radiology to specialists. Lab results move from clinics to primary care providers. Insurance claims flow between billing departments and payers. Patient records transfer between hospitals during referrals. Each of these transactions involves protected health information, and each represents a potential compliance failure if handled incorrectly.
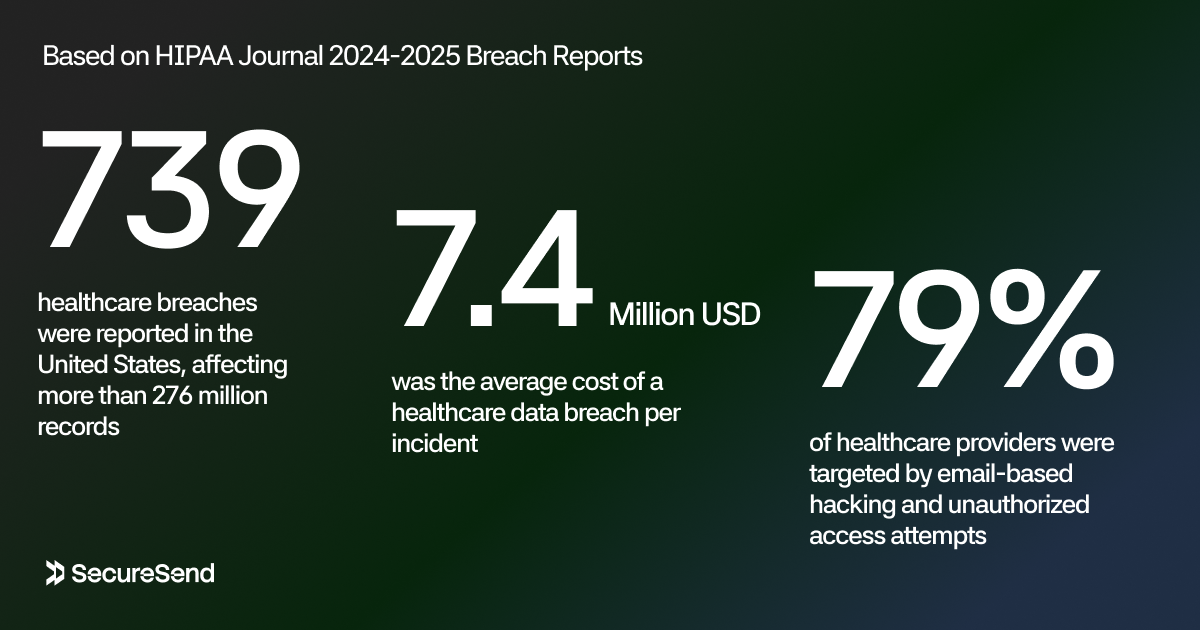
The numbers explain why this matters. In 2024, approximately 739 healthcare breaches were reported in the United States, affecting more than 276 million records. HIPAA Journal 2024-2025 Breach Reports put the average cost at $7.4 million per incident. Ransomware alone hit healthcare 458 times, with attackers demanding an average of $7 million.
Email-based attacks have become the dominant entry point. In 2024, 79 percent of healthcare providers were targeted by email-based hacking and unauthorized access attempts. Simulated phishing campaigns show that nearly 88 percent of healthcare workers click on malicious links, a staggering rate that reflects both the sophistication of modern attacks and the pressure of clinical workflows that leave little time for security vigilance.
File sharing sits at the center of this risk. Every time a nurse emails a patient summary to a specialist, every time a billing clerk uploads claims to a cloud folder, every time a researcher shares a de-identified dataset with a collaborator, the organization is either enforcing HIPAA safeguards or violating them. The channel matters. The controls matter. The documentation matters. And the regulators are watching.
What HIPAA Actually Requires for Electronic PHI
HIPAA compliance for file sharing starts with understanding what the law actually says. Three rules form the foundation: the Privacy Rule, the Security Rule, and the Breach Notification Rule. Together with the Business Associate provisions, they create a framework that every file sharing decision must navigate.
Protected Health Information and Electronic PHI
Protected health information, or PHI, is any individually identifiable information about a patient's past, present, or future physical or mental health, treatment, or payment for care. When that information exists in electronic form, it becomes electronic PHI, or ePHI. File sharing almost always involves ePHI. A PDF of a discharge summary, a DICOM image from a CT scan, a spreadsheet of billing codes, even a photograph of a wound for telemedicine consultation, all constitute ePHI when they contain identifiers that could link the data to a specific patient.
The Security Rule's Technical Safeguards
The HIPAA Security Rule at 45 CFR Part 164 Subpart C requires covered entities and business associates to implement administrative, physical, and technical safeguards to ensure confidentiality, integrity, and availability of ePHI. HHS Security Rule guidance provides the framework for these decisions.
Access control requires unique user identification, emergency access procedures, automatic logoff, and encryption mechanisms. In practical terms, this means no shared login credentials, session timeouts on shared workstations, and the ability to grant or revoke access based on role.
Audit controls demand mechanisms that record and examine activity in systems containing ePHI. Every upload, download, view, and permission change must be logged with user identity, timestamp, and action type. These logs must be retained for at least six years, and emerging guidance suggests seven years for access and modification logs.
Integrity safeguards protect ePHI from improper alteration or destruction. Checksums, cryptographic hashes, and digital signatures verify that a file has not been tampered with during transit or storage.
Person or entity authentication ensures that anyone seeking access to ePHI is who they claim to be. Passwords alone are no longer sufficient. Multi-factor authentication has become the expected standard.
Transmission security requires technical measures to guard against unauthorized access to ePHI when it is transmitted over electronic networks. This is where encryption in transit becomes non-negotiable.
The Breach Notification Rule and Encryption Safe Harbor
The Breach Notification Rule creates a powerful incentive to encrypt. Any impermissible use or disclosure of unsecured PHI is presumed to be a breach unless the organization can demonstrate a low probability that the PHI was compromised. However, if the PHI was encrypted in a manner consistent with guidance from the Secretary of Health and Human Services, and the decryption key was not also breached, the incident does not trigger breach notification obligations. This is the encryption safe harbor. Properly encrypted ePHI that is lost, stolen, or misdirected may not trigger breach notification obligations, saving the organization from the 60-day reporting timeline, individual notifications, HHS reporting, and media alerts for large breaches.
Business Associates and BAAs
Any vendor that creates, receives, maintains, or transmits PHI on behalf of a covered entity is a business associate. File sharing services, cloud storage providers, email platforms, and secure transfer tools all fall into this category. Before sharing PHI through any third-party service, the covered entity must obtain a signed Business Associate Agreement that specifies how the vendor will safeguard the information, what uses and disclosures are permitted, and how breaches will be reported. Without a BAA, using the vendor is itself a HIPAA violation, regardless of how strong the vendor's technical controls might be.
There is no official government registry of "HIPAA-approved" software. No vendor can legitimately claim to be "certified HIPAA compliant" by HHS. Compliance depends on how the organization configures the tool, manages access, maintains logs, trains staff, and governs the relationship through a proper BAA.
How Insecure File Sharing Creates HIPAA Violations
Despite clear requirements, many healthcare organizations still rely on file sharing methods that create compliance exposure. Understanding these failure modes helps explain why purpose-built secure sharing has become essential.
Email Attachments with Unencrypted PHI
Standard email remains the most common violation vector. When a clinician attaches a patient summary, lab result, or imaging report to an ordinary email, the message travels through multiple servers in plaintext unless additional encryption is layered on top. Even when TLS protects the transit between hops, the message and attachment are often stored in plaintext on mail servers and end-user devices. The sender has no visibility into whether the document was opened, forwarded, downloaded, or copied. If the recipient's account is compromised months later, every attachment ever sent to them is exposed.
Misaddressed emails are a constant risk. Autocomplete errors, similar names, and rushed workflows lead to PHI being sent to the wrong recipient. Once an email leaves the outbox, it cannot be recalled in any meaningful way. The breach has occurred, and the organization must assess whether notification is required.
Consumer Cloud Storage Without BAAs
Consumer-grade tools like Google Drive, Dropbox, and Microsoft OneDrive are convenient for collaboration, but they create multiple HIPAA problems. First, the free or personal tiers do not come with BAAs, making their use for PHI illegal under HIPAA. Second, even enterprise tiers that offer BAAs require the organization to configure permissions correctly, and misconfigured shared folders with "anyone with the link" access have caused numerous breaches. Third, these services hold the decryption keys, meaning their employees, legal processes, or infrastructure compromises can expose patient data.
Unencrypted Removable Media
USB drives, external hard drives, and CDs containing imaging studies or patient exports continue to circulate in healthcare environments. When these devices are unencrypted, lost, or stolen, the PHI they contain is fully exposed. The Security Rule's addressable implementation specifications for encryption of data at rest on portable devices have become effectively mandatory through enforcement precedent. Organizations that lose unencrypted USB drives containing thousands of patient records face both breach notification obligations and OCR enforcement action.
Legacy File Transfer Protocols
Plain FTP and unencrypted HTTP remain in use in some healthcare IT environments, particularly for automated transfers between systems. These protocols transmit data and credentials in cleartext, making them trivial to intercept. Even older implementations of FTPS or TLS with deprecated cipher suites can fall short of modern expectations. Regulators and security frameworks now explicitly require TLS 1.2 or higher with strong cipher suites for all ePHI transmission.
Shadow IT and Unsanctioned Tools
Clinicians and staff, frustrated by cumbersome official systems, frequently turn to unsanctioned tools for file sharing. Personal email accounts, consumer messaging apps, and unauthorized cloud services bypass IT controls, logging, and BAAs entirely. The 2025–2026 emergence of "shadow AI" has added a new dimension, with staff copying patient information into public generative AI tools for summarization or analysis, creating unauthorized disclosures to third-party systems without any BAA or security assessment.
The 2025–2026 Shift: Encryption and MFA Are Now Baseline
HIPAA's Security Rule originally described encryption as an "addressable" implementation specification, meaning organizations could evaluate whether it was reasonable and appropriate for their environment and adopt alternative measures if not. That era has ended. Through a combination of formal regulatory updates, enforcement precedent, and industry consensus, encryption and multi-factor authentication have become baseline expectations for all ePHI systems.
Encryption Is Now Effectively Mandatory
Multiple 2025–2026 analyses confirm that HHS and OCR have moved away from the addressable framing for encryption. Updated guidance now treats full-coverage encryption as a non-negotiable baseline for all ePHI, with no exceptions. AES-256 is widely cited as the minimum acceptable standard for data at rest. TLS 1.2 or 1.3 is required for data in transit. Older TLS versions and weak cipher suites are explicitly unacceptable.
This shift has enforcement teeth. OCR resolution agreements repeatedly cite the absence of encryption as a core deficiency, and the encryption safe harbor in the Breach Notification Rule creates a direct financial and reputational incentive to implement it fully. Organizations that encrypt properly may avoid all of these.
Multi-Factor Authentication Is Expected Everywhere
MFA has followed a similar trajectory. What was once a recommended practice is now an expected control for all workforce access to systems that create, receive, maintain, or transmit ePHI. This includes EHRs, imaging systems, email, file shares, cloud services, VPNs, and remote desktop tools. The 2025–2026 guidance emphasizes that cost or vendor limitations are no longer acceptable justifications for omitting MFA. Organizations are advised to prioritize MFA deployment first on EHRs, then on email, then on all other systems containing patient data.
For file sharing platforms, this means MFA must be enabled not only for administrators but for all staff users, and where possible for external users with ongoing access to PHI.
Audit Log Retention Has Extended
The retention period for audit logs has also tightened. While the Security Rule's documentation requirements have historically been associated with six-year retention, emerging 2026 guidance suggests seven years for ePHI access and modification logs. These logs must be automatically generated, tamper-evident, searchable, and exportable for OCR audits. Simply turning on logging is not enough. The logs must capture user IDs, timestamps, action types, data accessed, and IP addresses, and they must be stored in a separate secure system rather than within the application database itself.
The 72-Hour Restoration Benchmark
A new expectation has emerged around resilience. While not a specific regulatory citation in the original HIPAA text, the interpretation of "reasonable and appropriate" contingency planning has converged on a 72-hour restoration capability. After a ransomware attack, natural disaster, or system failure, organizations are expected to restore access to critical ePHI within approximately three days. This requires not just backups but tested restoration procedures, documented recovery steps, and the ability to maintain security controls during the recovery process.
Substance Use Disorder Records Now Fall Under HIPAA
A significant 2024–2026 regulatory change affects substance use disorder records. Previously governed by the more restrictive 42 CFR Part 2, SUD records are now being integrated into HIPAA's framework with heightened confidentiality protections. As of February 2026, HIPAA-covered entities must comply with new federal requirements that incorporate Part 2 protections for SUD treatment records, including more restrictive consent rules for disclosures and limits on the use of SUD records in legal proceedings without patient consent or a qualifying court order. For file sharing workflows, this means SUD information may require separate consent management, stricter access controls, and additional caution when sharing with external parties.
What HIPAA Compliant File Sharing Looks Like in Practice
Translating HIPAA requirements into file sharing capabilities reveals a clear set of features that separate compliant workflows from risky ones.
End-to-End Encryption, Not Just Transport Encryption
Transport encryption using TLS protects data while it moves across networks, but it leaves files readable on the server. End-to-end encryption ensures that files are encrypted on the sender's device before upload and remain encrypted until the recipient decrypts them locally. The server stores only ciphertext. Even a complete server compromise cannot expose patient data without the decryption keys.
This architecture, sometimes called zero-knowledge, aligns with HIPAA's confidentiality requirements and significantly reduces breach impact. If an attacker gains access to the file sharing infrastructure, they find encrypted blobs and no keys. The attack surface shrinks from "compromise the server, access everything" to "compromise the server, access nothing useful."
For healthcare organizations, end-to-end encryption provides the strongest technical foundation for sharing ePHI through third-party services, particularly when combined with proper BAAs and access controls.
Unique User Identification and Role-Based Access
Shared accounts are a HIPAA violation waiting to happen. Every user must have a unique identifier so that access can be tracked, attributed, and revoked when roles change. Role-based access control enforces the minimum necessary standard by limiting each user to the files and functions required for their specific duties. A radiology technician sees imaging studies. A billing clerk sees claims data. A researcher sees de-identified datasets. No one sees everything by default.
Multi-Factor Authentication for All Users
MFA must be enforced for every account with access to ePHI, including file sharing platforms. The most secure implementations use authenticator apps or hardware security keys rather than SMS, which remains vulnerable to SIM swapping and interception. For external recipients such as referral partners or patients, one-time verification codes sent via email or SMS can provide a practical MFA layer for link-based access.
Detailed Audit Logging
Every action on every file must be logged: who uploaded it, who viewed it, who downloaded it, when, from what IP address, and on what device. Failed access attempts must also be recorded. These logs must be retained for at least six years, with seven years increasingly expected, and stored in a tamper-evident manner that prevents alteration or deletion. Centralized log aggregation and SIEM integration enable real-time monitoring for suspicious patterns, such as unusual download volumes or access from unexpected locations.
Automatic Logoff and Session Management
Unattended sessions on shared clinical workstations are a persistent risk. File sharing platforms must enforce automatic logoff after periods of inactivity. Session management should also include the ability to revoke all active sessions for a user instantly when compromise is suspected or employment ends.
Secure Link Sharing with Granular Controls
Link-based sharing is practical for healthcare workflows, but it requires fine-grained controls to be HIPAA-aligned. Essential features include:
- Expiration dates that automatically deactivate links after a set timeframe
- Password protection with passwords communicated through separate channels
- Download restrictions that limit whether files can be saved locally
- View-only modes that prevent downloading, printing, or copying
- IP or domain restrictions that limit access to known networks
- One-time access links that self-destruct after a single use
- Instant revocation that allows administrators to deactivate links immediately
These controls operationalize the minimum necessary standard by ensuring that ePHI is accessible only for the specific purpose, timeframe, and recipients required.
Integrity Verification
Files must not be altered in transit or storage without detection. Cryptographic hashes, checksums, or digital signatures verify that a file received is identical to the file sent. This supports both the Security Rule's integrity requirements and clinical safety, ensuring that a diagnostic image or lab result has not been corrupted or tampered with during transfer.
Secure Deletion and Lifecycle Management
Temporary files, cached data, and intermediate storage generated during upload and download must be securely wiped after the transfer completes. Retention policies should ensure that files are stored only as long as necessary for clinical, legal, or operational purposes, then securely destroyed. Simply moving files to a recycle bin is not sufficient. Secure deletion requires overwriting or cryptographic erasure that prevents recovery.
Large File Support
Healthcare generates enormous files. High-resolution imaging studies, diagnostic videos, and genomic datasets can range from hundreds of megabytes to hundreds of gigabytes. A HIPAA-aligned file sharing solution must handle these sizes without timeouts, corruption, or the need for staff to resort to unsanctioned workarounds.
Business Associate Agreements: The Contract That Makes It Legal
Technical controls are necessary but not sufficient. The Business Associate Agreement is what transforms a secure file sharing tool from a potential liability into a compliant component of your program.
Under 45 CFR §§ 164.502(e) and 164.504(e), covered entities must obtain satisfactory assurances that business associates will appropriately safeguard PHI. The BAA must specify permitted uses and disclosures, prohibit unauthorized uses, require implementation of Security Rule safeguards, and obligate the business associate to report breaches in a timely manner. If the business associate uses subcontractors that also handle PHI, the BAA must require equivalent agreements downstream.
For file sharing vendors, the BAA should explicitly address:
- Encryption standards for data at rest and in transit
- Access control and MFA requirements
- Audit logging and retention obligations
- Breach notification timelines and procedures
- Subcontractor management and downstream BAAs
- Data deletion and return procedures upon contract termination
- Permitted and prohibited uses of PHI
No BAA means no compliant sharing, no matter how strong the encryption. Organizations that use cloud storage, email services, or file transfer platforms without signed BAAs have committed a HIPAA violation before a single file is transmitted.
Real-World Healthcare File Sharing Scenarios
Theory matters less than practice. Here are specific situations where secure file sharing transforms compliance risk into controlled, auditable workflow.
Sharing Imaging Studies with External Specialists
A primary care physician needs to send a patient's MRI to a neurologist for consultation. The file is 800 megabytes, far too large for standard email. The physician uploads the study to a secure sharing platform with end-to-end encryption, generates a link valid for 72 hours, and sends it to the neurologist's verified email address. The neurologist authenticates with MFA, views the images in their browser, and the link expires automatically. The platform logs every access with user identity, timestamp, and IP address. No PHI sits in email inboxes. No unencrypted copy remains on consumer cloud servers. The audit trail documents the disclosure for compliance.
Transmitting Lab Results to Patients
A patient requests copies of their recent blood work under HIPAA's right of access. The clinic uploads the lab report to a secure portal, generates a password-protected link, and sends it to the patient's verified email. The patient receives the password via SMS. The link expires after seven days. The clinic's access log records the upload, the notification, and any views or downloads. If the patient needs more time, a new link is generated. The original report remains in the clinic's encrypted repository with full audit history.
Exchanging Claims Data with Payers
A hospital's billing department must submit claims documentation to multiple insurance payers. Each submission contains patient identifiers, diagnosis codes, procedure details, and financial information. Using a secure file sharing platform with role-based access, the billing team uploads each claim to a payer-specific folder with automatic expiration. Payer representatives access only their assigned claims through MFA-protected accounts. Audit trails document every download for dispute resolution and compliance. When a contract with a payer ends, access to their folder is revoked instantly.
Collaborating on Research Datasets
A research team needs to share a de-identified dataset with a university partner. The dataset has been stripped of direct identifiers but still contains dates of service and geographic data that could enable re-identification in combination with other sources. The team uploads the dataset through a secure platform with end-to-end encryption, shares a view-only link with the research partner, and restricts downloads. The link expires when the collaboration ends. Access logs support the data use agreement and institutional review board requirements.
FAQ: Common Questions About HIPAA and File Sharing
Is there a government-certified list of HIPAA compliant file sharing tools?
No. HHS does not certify, approve, or maintain a registry of HIPAA-compliant software. Compliance depends on how the tool is configured, governed, and used within your organization's broader program. A vendor can provide the technical controls, but your organization is responsible for implementing access policies, signing BAAs, training staff, and maintaining audit documentation.
Can I use email to send PHI if my organization has a secure email gateway?
Secure email gateways that encrypt messages can support HIPAA-compliant email, but they must be properly configured, covered by a BAA, and integrated with your logging systems. Standard email without encryption is not appropriate for PHI. Even with secure email, consider whether link-based sharing with expiration provides stronger protection.
What encryption standards does HIPAA require?
While HIPAA does not mandate specific algorithms, NIST guidance and industry consensus point to AES-256 for data at rest and TLS 1.2 or 1.3 for data in transit. Older protocols such as TLS 1.0, 1.1, and unencrypted FTP or HTTP are no longer acceptable for ePHI.
Does end-to-end encryption alone make file sharing HIPAA compliant?
No. End-to-end encryption is a powerful technical control that supports confidentiality and can provide breach notification safe harbor, but HIPAA compliance requires the full set of Security Rule safeguards: access controls, audit logging, integrity verification, authentication, and transmission security, plus administrative safeguards like risk analysis, training, and BAAs. End-to-end encryption is a critical component, not a complete solution.
How long must we retain file sharing audit logs?
The Security Rule requires documentation retention for six years from creation or last effective date. For audit logs specifically, emerging 2026 guidance suggests retaining ePHI access and modification logs for seven years. Logs must be automatically generated, tamper-evident, and searchable for OCR audits.
What happens if we share PHI through a vendor without a BAA?
Sharing PHI with a business associate without a signed BAA is a HIPAA violation, regardless of the vendor's technical security. OCR enforcement actions have repeatedly cited missing BAAs as a primary deficiency. If a breach occurs through an uncontracted vendor, the covered entity faces both the breach notification obligations and enforcement action for the BAA failure itself.
Are consumer cloud storage services like Google Drive or Dropbox ever acceptable for PHI?
Only if the organization has a signed BAA with the vendor and uses an enterprise tier with HIPAA-aligned controls. Free or personal tiers do not come with BAAs and must not be used for PHI. Even enterprise tiers require active configuration to prevent misconfigured access.
What should we do if we suspect a file was shared inappropriately?
If shared through a secure platform, revoke the link immediately and review access logs. Document your response actions. Notify your security coordinator. Assess whether the incident constitutes a breach. If the file contained ePHI and was disclosed without authorization, you may have 60 days to notify affected individuals and HHS unless you can demonstrate a low probability of compromise.
Conclusion: File Sharing Is Part of Your Compliance Program
HIPAA compliance is a program you build, maintain, and document across every system that touches patient data. It is not a product you purchase. File sharing is one of the most active and vulnerable components of that program because it is where ePHI leaves the controlled environment of your EHR or imaging system and enters the broader digital ecosystem.
The requirements are clear. Encrypt ePHI at rest and in transit. Authenticate every user with unique credentials and multi-factor verification. Log every access with enough detail to reconstruct what happened. Enforce the minimum necessary standard through role-based permissions and time-limited access. Sign BAAs with every vendor that handles PHI. Train your staff to use sanctioned tools and recognize the workarounds that create exposure. Test your backups and restoration procedures. And document everything, because when OCR comes calling, your records are your defense.
The threat environment has made these controls non-negotiable. Ransomware groups target healthcare because patient data is valuable and disruption is deadly. Phishing campaigns exploit busy clinicians who need to move information quickly. Regulators have responded by tightening expectations around encryption, MFA, and logging, with enforcement actions that now routinely reach into the millions of dollars.
Secure file sharing platforms that provide end-to-end encryption, granular access controls, detailed audit trails, and link-based sharing with expiration and revocation give healthcare organizations the technical foundation to meet these requirements without sacrificing the speed and collaboration that patient care demands. When integrated into a broader compliance program with proper BAAs, policies, training, and governance, they transform file sharing from a compliance risk into a controlled, auditable, and defensible workflow.
Your patients trust you with their most sensitive information. That trust deserves more than an email attachment or an open cloud folder.
Ready to protect patient data with end-to-end encrypted file sharing, granular access controls, and complete audit trails? Create your first secure file sharing link with SecureSend and experience secure document sharing built for healthcare workflows.
Sources: HHS Office for Civil Rights, HIPAA Journal 2024–2025 Breach Reports, IBM Cost of Data Breach Report 2025, 45 CFR Part 164, 42 CFR Part 2, NIST SP 800-66.